Thinking Outside the Beta-Amyloid Box
The dominant amyloid hypothesis of AD has translated into an armada of anti-amyloid biologics in the near-term pipeline—led by Eisai and Biogen’s lecanemab. Last month, lecanemab showed a slowing in the rate of cognitive decline by 27% over 18 months versus placebo. Lecanemab also possesses a relatively improved safety profile among the beta-amyloid mAbs, as a result of lower rates of amyloid-related imaging abnormalities (ARIA) (this was a significant issue with aducanumab). This improved safety profile eliminates the need for a dose titration period. The other notable beta-amyloid mAb drug contenders include Roche’s gantenerumab and Eli Lilly’s donanemab, which may achieve the fastest amyloid plaque clearance among its competitors.
These recent successes, however, come after an approximate 98% failure rate in phase 2 and 3 trials since 2003.1 For a disease that kills more people than breast cancer and prostate cancer combined,2 a modest improvement in cognitive decline is not enough. This has led many labs to pursue other potential targets in AD, with some encouraging early signals of success (Table 1).3
Table 1. Alzheimer’s drug development pipeline: disease-modifying drug candidates with non-amyloid mechanisms of action with corporate sponsor in phase 2 and 3 and select phase 1 drug candidates, grouped by target. Source: Cummings et al (2022).3
| Sponsor | Drug candidate | Target | Trial status |
|---|---|---|---|
| Vigil Neuro | VGL101 | TREM2 | Phase 1 |
| Denali Therapeutics Inc. | DNL919 | TREM2 | Phase 1 |
| TauRx Therapeutics | TRx0237 | Tau | Phase 3; active |
| AC Immune, Janssen | ACI-35 | Tau | Phase 2; recruiting |
| UCB Biopharma | Bepranemab | Tau | Phase 2; recruiting |
| Eisai | E2814 | Tau | Phase 2; recruiting |
| Ionis Pharmaceuticals | IONIS MAPTRx (BIIB080) | Tau | Phase 2; active |
| Janssen | JNJ-63733657 | Tau | Phase 2; recruiting |
| Eli Lilly | LY3372689 | Tau | Phase 2; recruiting |
| Samus Therapeutics | PU-AD | Tau | Phase 2; active |
| Genentech | Semorinemab (R07105705) | Tau | Phase 2; active |
| AgeneBio, NIA | AGB101 | Synaptic plasticity | Phase 3; active |
| Cortexyme | Atuzaginstat (COR388) | Synaptic plasticity | Phase 3; active |
| Anavex Life Sciences | Blarcamesine (ANAVEX2-73 | Synaptic plasticity | Phase 3; active |
| Cassava Sciences | Simufilam (PTI-125) | Synaptic plasticity | Phase 3; recruiting |
| Tetra Discovery Partners | BPN14770 | Synaptic plasticity | Phase 2; active |
| Neurotrope Bioscience, NIH, NIA | Bryostatin 1 | Synaptic plasticity | Phase 2; recruiting |
| Cyclerion Therapeutics | CY6463 | Synaptic plasticity | Phase 2; recruiting |
| Toyama Chemical | Edonerpic (T-817MA) | Synaptic plasticity | Phase 2; active |
| Cognition Therapeutics | Elayta (CT1812) | Synaptic plasticity | Phase 2; recruiting |
| Athira Pharma | Fosgonimeton (ATH-1017) | Synaptic plasticity | Phase 2; recruiting |
| Neurokine Therapeutics, et al. | MW150 | Synaptic plasticity | Phase 2 |
| EIP Pharma | Neflamapimod (VX-745) | Synaptic plasticity | Phase 2; recruiting |
| Biohaven Pharma, ADCS | Troriluzole (BHV4157) | Synaptic plasticity | Phase 2; active |
| KeifeRx | Nilotinib BE | Proteostasis/ proteinopathies | Phase 3 |
| QR Pharma, ADCS | Posiphen | Proteostasis/ proteinopathies | |
| Pharmazz | Sovateltide (PMZ-1620) | Neurogenesis | Phase 2; recruiting |
| Novo Nordisk | Semaglutinide | Metabolism and bioenergetics | Phase 3; recruiting |
| Cerecin | Tricaprilin | Metabolism and bioenergetics | Phase 3 |
| T3D Therapeutics, et al. | T3D-959 | Metabolism and bioenergetics | Phase 2; recruiting |
| NewAmsterdam Pharma | Obicetrapib | Lipids and lipoprotein receptors | Phase 2 |
| Neurmedix | NE3107 | Inflammation | Phase 3; recruiting |
| Alector, AbbVie | AL002 | Inflammation | Phase 2; recruiting |
| Novartis | Canakinumab | Inflammation | Phase 2; recruiting |
| GMP BIO, BHT Lifescience Australia | GB301 | Inflammation | Phase 2 |
| IntelGenx Corp. | Montelukast | Inflammation | Phase 2; recruiting |
| Vaccinex, ADDF, Alzheimer’s Association | Pepinemab (VX15) | Inflammation | Phase 2; recruiting |
| TrueBinding, Inc | TB006 | Inflammation | Phase 2; recruiting |
| Mindful Diagnostics and Therapeutics | Tdap vaccine | Inflammation | Phase 2 |
| Northwell Health, Janssen | Daratumumab | Inflammation | Phase 2; recruiting |
| Shanghai Green Valley | GV-971 | Gut-brain axis | Phase 3; recruiting |
| Actinogen Medical | Xanamem | Growth factors and hormones | Phase 2; active |
| GemVax & Kael | GV1001 | Epigenetic | Phase 2 |
| Neuroscience Trials Australia | Deferiprone | Cell death | Phase 2; active |
The AD therapeutic landscape appears to be shifting away from symptomatic drugs and focusing more on disease-modifying drugs (DMDs)—a report by the Alzheimer’s Association (AA) showed that 68% of agents in phase 3 trials are DMDs (Figure 2).3 Most of these DMDs target beta-amyloid (29%); however, the remainder represent innovative new directions in targeting the multifactorial, complex pathology of AD.
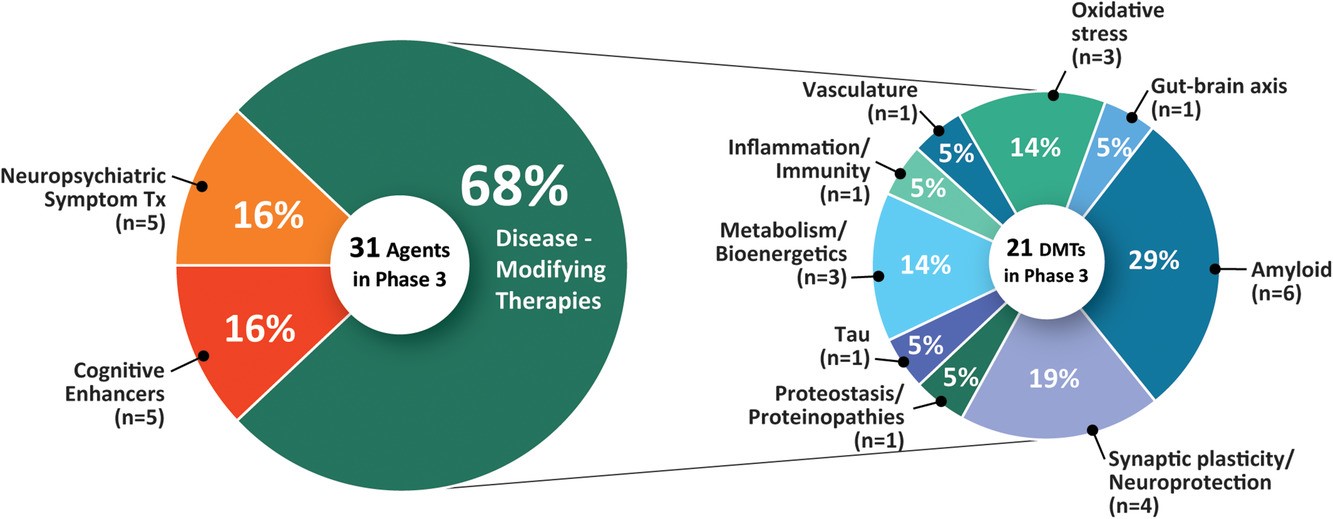
Figure 2. Mechanisms of action of agents in phase 3.3
The discovery that mutations in “triggering receptor expressed on myeloid cells 2” (TREM2) can increase the risk of AD by up to threefold, suggested the involvement of inflammatory pathology in AD.4-6 TREM2 is a transmembrane protein located on the surface of microglia, the resident immune cells of the brain. Microglia are dynamic, innate immune cells of the brain: functioning to constantly sense extracellular cues (e.g., cellular debris, invading viruses or bacteria) in the central nervous system (CNS). In the absence of extracellular cues, the microglia are in a homeostatic conformation. When cellular debris binds to TREM2, homeostatic microglia are activated and transition to disease-associated microglia (DAM). Microglia in the DAM state also function to clear proteins that aggregate in neurodegenerative diseases—such as amyloid plaques in AD. Because TREM2 loss-of-function mutations are associated with the inability of microglia to transition to the DAM phenotype, they are a rational target in AD. Dysfunctional microglia expressing mutated TREM2 are unable to clear cellular debris, and this leads to a perpetuation of neuroinflammation and subsequent neurodegeneration.
Further research bridging pathologies has revealed that TREM2 biology directly involves beta‑amyloid: TREM2 binds to beta-amyloid, and this binding is compromised in the presence of AD‑associated mutations.7 Moreover, TREM2 has been linked to the long-established genetic risk factor of the late-onset (after age 60) form of AD: the ε4 allele of apolipoprotein E (APOE).8
Targeting TREM2 is particularly attractive because it is restricted to the area of pathology—the brain. Denali Therapeutics’ TREM2-targeted therapy, DNL919, uses a proprietary antibody delivery technology to deliver drug across the protective blood-brain barrier and activate the receptor. DNL919 was this year placed on a clinical hold before it entered human trials due to issues surrounding the preclinical toxicology assessment. Denali is working to provide the FDA with the information needed to restart the clinical trial.
Massachusetts-based Vigil Neuro is developing disease-modifying therapeutics to restore the microglia DAM phenotype by activating TREM2 signaling in order to treat neurodegenerative diseases such as AD. Vigil is targeting the activation of TREM2 with VGL101, a drug currently in a phase 1 healthy volunteer trial that is slated to read out by the end of the year.
The potential role of gut microbiota in AD pathogenesis9 has culminated in the discovery of a plant-based compound, sodium oligomannate (GV-971), by Shanghai Green Valley Pharmaceutical. GV-971 contains an active ingredient derived from brown algae and was recently shown to therapeutically remodel gut microbiota, resulting in the suppression of inflammation and inhibition of AD progression10. China’s drug regulator approved marketing of GV-971 following encouraging results from a 36-week phase 3, multicenter, randomized, double-blind, placebo-controlled parallel-group clinical that revealed significant improvements in cognition.
Deficits in axonal transport—a cellular process that mediates the movement of diverse cargoes along axons—has been shown to be a contributing pathology in the neurodegeneration seen in AD (as well as other neurological diseases).11,12 Buntanetap, a drug being developed by Annovis Bio, inhibits multiple neurotoxic aggregating proteins—including beta-amyloid, tau, α-synuclein and TAR DNA-binding protein 43 (TDP-43)—to restore axonal transport to normal levels. Annovis recently reported positive safety data and a statistically significant improvement in cognition from its phase 2a Alzheimer’s study, and this month received FDA authorization to initiate a phase 2/3 clinical trial of buntanetap in moderate AD.
It appears that the AD field is now refocusing on pathologies outside of aberrant amyloid and tau protein, and looking more closely at diverse biological processes including inflammatory cascades, gut-brain signaling, and axonal transport. It’s likely that ongoing translational research will eventually lead to a better understanding of these diverse pathologies and that overall treatment of AD will ultimately be multifactorial.
 Muzamil Saleem, PhD
Muzamil Saleem, PhD
Associate Scientific Director, ProEd Regulatory
Muz is a trained neuroscientist with a diverse skillset, combining a ten-year neurology-focused research career, scientific consulting experience and a three-year tenure in healthcare equity research on Wall Street before joining ProEd Regulatory—all supported by a passion for written and visual scientific communication. Connect with Muz on LinkedIn.
References
- Kim CK, Lee YR, Ong L, Gold M, Kalali A, Sarkar J. Alzheimer’s Disease: Key Insights from Two Decades of Clinical Trial Failures. J Alzheimers Dis. 2022;87(1):83-100.
- 2022 Alzheimer’s disease facts and figures. Alzheimers Dement. 2022;18(4):700-789.
- Cummings J, Lee G, Nahed P, et al. Alzheimer’s disease drug development pipeline: 2022. Alzheimers Dement (N Y). 2022;8(1):e12295.
- Guerreiro R, Wojtas A, Bras J, et al. TREM2 variants in Alzheimer’s disease. N Engl J Med. 2013;368(2):117-127.
- Ulland TK, Colonna M. TREM2 – a key player in microglial biology and Alzheimer disease. Nat Rev Neurol. 2018;14(11):667-675.
- Qin Q, Teng Z, Liu C, Li Q, Yin Y, Tang Y. TREM2, microglia, and Alzheimer’s disease. Mech Ageing Dev. 2021;195:111438.
- Zhao Y, Wu X, Li X, et al. TREM2 Is a Receptor for beta-Amyloid that Mediates Microglial Function. Neuron. 2018;97(5):1023-1031 e1027.
- Fitz NF, Wolfe CM, Playso BE, et al. Trem2 deficiency differentially affects phenotype and transcriptome of human APOE3 and APOE4 mice. Mol Neurodegener. 2020;15(1):41.
- Varesi A, Pierella E, Romeo M, et al. The Potential Role of Gut Microbiota in Alzheimer’s Disease: From Diagnosis to Treatment. Nutrients. 2022;14(3).
- Wang X, Sun G, Feng T, et al. Sodium oligomannate therapeutically remodels gut microbiota and suppresses gut bacterial amino acids-shaped neuroinflammation to inhibit Alzheimer’s disease progression. Cell Res. 2019;29(10):787-803.
- Millecamps S, Julien JP. Axonal transport deficits and neurodegenerative diseases. Nat Rev Neurosci. 2013;14(3):161-176.
- Guo W, Stoklund Dittlau K, Van Den Bosch L. Axonal transport defects and neurodegeneration: Molecular mechanisms and therapeutic implications. Semin Cell Dev Biol. 2020;99:133-150.